Everyone experiences occasional aches and pains. In fact, sudden pain is an important reaction of the nervous system that helps alert you to possible injury – it is a protective mechanism. When an injury occurs, pain signals travel from the injured area, up your spinal cord, and to your brain. It is a simple reaction.
However, chronic pain is more complex with the involvement of psychosocial factors and multiple biological issues. As human beings, all of us, and sometimes even doctors, forget the difference between acute and chronic pain.
These are 2 entirely different concepts. Acute pain is something you experience on a daily basis. Examples would be when you put a finger on a hot stove, somebody puts their foot on your toe, you unconsciously hit your elbow, you have a kidney stone, or give birth. Acute pain means that there is something wrong with your body and it needs to be corrected. But chronic pain is long-lasting. It continues after normal healing has occurred or should have occurred. Occasionally chronic pain becomes a disease in itself. In chronic pain, signals travel from the painful area up the spinal cord and the brain as in acute pain. However, there are multiple factors amplifying this pain. For these reasons, many patients develop allodynia (experience of pain from stimuli that isn’t normally painful) and hyperalgesia (experience of enhanced sensitivity to pain).
Generally, we believe that chronic or persistent pain is pain lasting for 6 months or longer that does not respond to traditional medical or surgical treatment. Some even believe it to be just 3 months. Please remember, chronic pain may be there and you may still have acute episodes in the same region or acute pain that is unrelated to your chronic pain.
Each specialty in medicine has an official definition. These definitions come from an organization called the National Uniform Claims Committee. As with other specialties, this committee derived the definition for interventional pain management after consulting with scientists, physicians, patients, and health policymakers.
In layman’s terms, interventional pain management is a specialty of medicine concentrating on the diagnosis and treatment of pain by applying various types of treatments, but mainly interventional techniques. These interventional techniques not only manage difficult cases but occasionally simple cases. Ones where surgery is not indicated or other methods have failed to identify the cause of pain, even when using traditional testing methods like physical examination, x-rays, MRI and CT scanning, as well as nerve conduction studies.
In interventional pain management settings, the pain is treated with a combination of various techniques which address multiple conditions when other types of treatments have failed to provide significant improvement. We apply all traditional techniques including physical therapy, education and behavior modification, drug therapy, and structured exercise programs. All traditional techniques are applied in conjunction with interventional techniques to provide maximum effect, or you may say “best bang for the buck.”
As interventional pain physicians, similar to other physicians, we have many goals. While our major goal appears to be to relieve the pain, but it is relief of the pain in conjunction with function. Of course, the most successful patient is one who goes back to work, enjoys family life, and does not use any medications.
In many cases, as you well know, that is not achievable. The majority of patients who come to us consider us as their last hope. They have seen many doctors, had surgeries, and in the majority of cases, they are already disabled. Chronic, persistent intractable pain is a condition that might not be cured. We can only cure pain in some cases, but in the majority of cases, we can manage it. Our dictum is to improve the quality of life by reducing pain to a tolerable level and increasing function so that you can enjoy life and carry on activities of daily living even though sometimes they may be very simple such as going to the bathroom, grocery store, playing with kids or grandkids.
In medicine there are many specialties such as primary care physician, cardiologist, orthopedic surgeon, and many others. Interventional pain specialists are educated and trained to treat chronic, persistent pain. You should look for an interventional pain physician who has special qualifications, such as fellowship training or board certification in pain medicine. A relationship with a pain physician is long-lasting, or even life-long. You should check to see if the physician can make independent decisions without influence from others. Also, make sure when a physician leaves town or your insurance changes, you will still be covered. Chronic pain is very complex. It is difficult to diagnose and treat. An interventional pain physician uses many tools to diagnose the exact cause of your pain. One of the most important tools is you, the patient. It is important that you describe not only where the pain is, but also what kind of pain it is, how it started, and what effect it has on your life. This gives your interventional pain physician the clues needed to make an accurate diagnosis and treatment plan. Remember: A doctor who cannot take a good history and a patient who cannot give one are in danger of giving and receiving bad treatment.
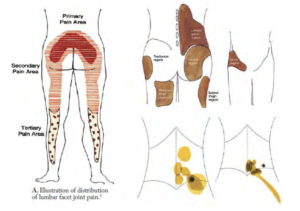
FIGURE 1. REFERRED PAIN
Referred pain or somatic pain typically from facet joints or discs is limited to the low back or neck with some pain felt in the extremities which is deep, bony, throbbing, and aching. 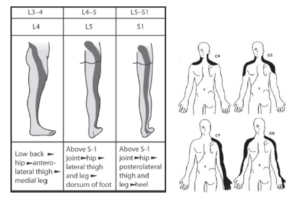
FIGURE 2. RADICULAR PAIN
In contrast, radicular pain predominantly in the extremities, due to nerve root irritation is sharp, shooting, like an electric shock which can be traced with a superficial line in the skin.
Many people think that pain is a diagnosis, but this is not true. Pain is a symptom that tells the physician that something is wrong. When a physician finds out what is wrong, then the physician can treat the cause of the pain. During your appointment with the pain management physician, they will take a medical history from you, focusing on your pain, and review or order appropriate tests. Even then, the physician may not be able to pinpoint your pain’s cause. Diagnostic nerve blocks improve our ability to pinpoint a diagnosis so an individual treatment plan can be created for you.
Structures causing pain in the spine can be identified in only approximately 20% of the patients based on history and various tests including MRI and nerve conduction studies. Correct diagnosis is extremely important for proper management. We can identify the proper source of pain by injecting small doses of local anesthetic into the area of the nerve supply and evaluating the patient for appropriate relief based on accepted criteria. Diagnostic nerve blocks can help an interventional pain physician to pinpoint the source of pain and make a diagnosis and provide appropriate treatment.
Facet joint pain is one of the most common pain symptoms with neck, mid-back, and low back pain. These major structures in the spine, on each side of a vertebral body, allow us to bend forward, backward, and side to side. Facet joints can cause pain secondary to arthritis, degeneration, and also sprain and strain. Facet joint pain is typically limited to the low back, mid back, or neck with some radiation into the extremities. Facet joint pain is deep, bony, throbbing, and aching, rather than sharp or shooting, like an electric shock or radicular pain. Facet joint pain can be diagnosed with a history, physical examination, and x-rays, but most importantly with diagnostic facet joint nerve blocks.
Facet joint nerve blocks are also known as medial branch blocks and are performed by placing a small needle over the nerve supply of the joint and injecting a local anesthetic. If facet joint pain is confirmed, further treatment can involve repeat injections once in 3 to 6 months with therapeutic medial facet joint nerve blocks or once in 6 months to a year with radiofrequency neurotomy, or application of heat to the nerves. An interventional pain physician can make the diagnosis of facet joint pain and manage the pain, reduce pain, increase function, and help make life easier to live.
Low back and lower extremity pain are the most common chronic pain problems. The low back is known as the lumbosacral region of the spine with 5 lumbar vertebrae labeled from L1 to L5 and one S1 vertebral body. They are between the thoracic, or chest, region of the spine and the sacrum. Lumbosacral vertebrae are connected by 2 facet joints on each side which allow for forward and backward extension as well as twisting movements. Facet joints may cause pain due to degeneration, arthritis, sprain, and strain.
In addition to the facet joints at each vertebral level, there is a disc in between the vertebrae providing support. The discs are like jelly donuts. These discs in the lumbar region are most likely to degenerate, bulge, protrude, or herniate and may irritate nerves causing low back and lower extremity pain.
The spinal cord mostly ends at T12 and L1 where the thoracic spine meets the lumbar spine. From there on, nerve roots branch out from the spinal cord forming what is known as the cauda equina or horse’s tail. Arthritis can develop in any part of the spine including the facet joints, leading to spinal stenosis or facet joint arthritis. The lumbar spine includes an intricate network of muscles, tendons, and ligaments that provide support and movements. These tissues can become strained and produce spasm causing low back pain, hip pain, groin pain, and occasionally leg pain associated with stiffness.
The bones in our spine are called vertebrae. They are separated from each other by discs which are like jelly donuts and act as cushions between the bones. Not only can these discs be a source of pain, they can also cause pain by pressing up against a nerve. Various levels of disc displacement are: disc bulging, disc protrusion, disc herniation, and disc extrusion.
A bulging disc occurs when the tough outer part of the disc, called the annulus, compresses and squeezes out. A herniated disc, also called a ruptured disc, is when the inner nucleus leaks through a crack in the annulus. Normal aging or an injury can cause either of these to happen, but they are treatable conditions.
All these medical terms basically mean that the disc is sticking out beyond where it is supposed to be. The nerves are irritated due to pressure or the irritating chemicals released from the disc. An Interventional Pain Physician can make the diagnosis based on your history, physical examination, and radiologic findings, and also treat appropriately
Pain in the neck is common, second only to pain in the low back. The cervical spine or neck starts at the base of the skull and through a series of 7 vertebral segments connect to the thoracic region of the spine.
Among the 7 cervical vertebrae, the first two are extremely unique, providing most of the rotation of the neck and the head.
The 7 vertebrae of the cervical spine are connected in the back by 2 facet joints, one on each side, which allow for forward and backward extensions, as well as twisting movements.
In between the vertebrae are 6 cervical discs that act as shock absorbers and also allow for flexibility and movement of the neck. The cervical spine has 8 cervical nerves from C1 through C8, that branch off of the spinal cord and exit through the neural foreman in the back of the spine.
The facet joints, discs, and nerve roots can be responsible for pain in the neck, headaches, and pain in the upper extremities and occasionally into the chest wall. The discs may degenerate, irritating the nerves, but they also may bulge, protrude, or herniate with wear and tear over time or from an injury, thus causing pain. Arthritis can develop in any part of the spine including the facet joints, leading to spinal stenosis or facet joint arthritis.
The sacroiliac joint is a major joint in the human body and connects the sacrum, the triangular bone at the bottom of the spine, with the pelvis, also known as the iliac bone, which is the part of the hip joint on each side of the lower spine. It is not clear why and how sacroiliac joint dysfunction occurs. Sacroiliac joint pain typically results in pain on one side very low in the back, in the buttocks, in the groin, in the hip, or in the lower extremity.
Sacroiliac joint pain may be secondary to inflammation or sacroiliitis, other traumatic incidents, or after lumbar surgery. Rehabilitation therapy and non–steroidal anti-inflammatory drugs are provided as the first line treatment for sacroiliac joint pain.
Sacroiliac joint injections or SI joint injections are used to diagnose and treat low back pain symptoms. Radiofrequency nerve ablation is also performed for long-term relief.
Fibromyalgia syndrome is a common and chronic disorder with widespread musculoskeletal pain associated with fatigue, sleep, memory, and mood issues. Researchers believe that fibromyalgia amplifies painful sensations by affecting the way the brain processes pain signals. In the majority of cases, symptoms gradually accumulate over time with no single triggering event.
Women are much more likely to develop fibromyalgia than are men.
Cognitive and memory problems associated with fibromyalgia have been described as fibro fog.
A fibromyalgia diagnosis is based on a history of widespread pain lasting more than 3 months.
Unfortunately, patients suffering with fibromyalgia may also suffer with multiple other problems, including spinal pain or neuropathic pain. They also may have depression, anxiety, and other psychological problems.
Fibromyalgia may be treated with medical therapy, behavior modification, rehabilitation modalities, and by improving sleep. Only 3 medications, Cymbalta, Savella, and Lyrica, are approved by the U.S. Food and Drug Administration for the treatment of fibromyalgia. Neurontin is also commonly used in fibromyalgia.
Post herpetic neuralgia is a condition that produces severe, agonizing pain and suffering for many patients following the viral infection called herpes zoster, most commonly known as shingles. This painful condition may last several months to years.
Shingles or herpes zoster is an acute viral infection affecting the skin and nerves which show up as small blisters appearing along certain nerve segments. Shingles most commonly occur in individuals with reduced defense mechanisms to fight infection by re–activation of the chickenpox virus which was inactive. It most commonly affects the chest wall and upper back in 50% of cases, neck and upper limbs in 20% of cases, lower back and lower limb in 15% of cases, and the eye in 15% of cases. This disease mainly involves a nerve root ganglion, a collection of nerve tissue that may be replaced by scar tissue. This scar tissue may be the cause of various problems, one being reducing the diameter of the blood vessels. Another reason is that there is unequal damage of large diameter nerve fibers over small fibers. This changes the balance and allows the brain to transmit pain impulses without obstruction.
The main drugs used for managing shingles is neuropathic drugs such as gabapentin, or Neurontin, and pregabalin, or Lyrica. Some patients may be candidates for injection therapy with sympathetic blocks or epidural injections or other nerve blocks. An interventional pain physician can make an appropriate diagnosis and provide treatment to reduce pain, increase function, and help make life easier to live.
Complex regional pain syndrome, or CRPS, is also known as reflex sympathetic dystrophy, or RSD, or causalgia. The pain from CRPS usually affects one or more of the extremities. CRPS pain is often described as constant and intense, generally out of proportion with the original injury. CRPS also can cause a change in skin temperature, color, or texture, along with extreme skin sensitivity and swelling or stiffness of the affected area. CRPS often develops after a minor injury or trauma such as an ankle or wrist fracture or surgery, affecting the nerves, muscles, and tendons. Currently there is no single diagnostic test to confirm CRPS. Consequently, careful examination and assessment is important. Magnetic resonance imaging (MRI) or a triple-phase bone scan sometimes identifies CRPS changes in bone metabolism.
Multiple drugs used in managing CRPS are the same drugs used in neuropathic pain such as gabapentin, or Neurontin, amitriptyline, nortriptyline, and pregabalin, or Lyrica. Sympathetic nerve block is one of the management modalities for moderate to severe cases that do not respond to reha–bilitation and medication therapy. Sympathetic blocks provide gradual pain relief by blocking sympathetic nerves. The procedure involves injecting an anesthetic next to the spine to directly block the activity of sympathetic nerves and improve blood flow based on the location of the pain, either the upper extremity or the lower extremity. If all else fails, a ketamine infusion or spinal cord stimulation may be considered.
Neuropathic pain involves the central nervous system, which includes the brain and spinal cord, or the peripheral nerve system, which includes all the other nerves. The pain may be continuous or intermittent, described as stabbing, electric shocks, pins and needles, burning or cold sensations, numbness and itching. Neuropathic pain may affect as many as 5% to 10% of the population.
Central neuropathic pain is commonly found in spinal cord injury, multiple sclerosis, and some strokes. Peripheral neuropathic pain is secondary to diabetic neuropathy, herpes zoster infections, or shingles, HIV-related infections, nutritional deficiencies, toxins, and trauma to the nerve trunk. Neuropathic pain is also very common in cancer. It also may be associated with chemotherapy, radiation therapy, or surgery. Neuropathic pain may be very difficult to treat with less than 50% of people achieving some relief. Most common treatments are some antidepressant medications and antiepileptic drugs including Neurontin and Lyrica.
An interventional pain physician can diagnose neuropathic pain and treat to reduce pain, increase function, and help make life easier to live.
Nonsteroidal anti-inflammatory drugs, also known as NSAIDs, provide pain relief and reduce fever and in higher doses provide anti-inflammatory effects. Some of these are available over the counter such as aspirin, Advil, and Aleve. Others are prescription drugs. NSAIDs are used for the treatment of a wide variety of acute and chronic painful conditions, specifically when there is inflam–mation. They are very safe drugs, but have significant side effects with gastrointestinal irritation, bleeding, or even death. NSAIDs can also cause kidney and cardiovascular problems. In July 2015, the FDA toughened its warnings concerning the increased risk of heart attack and stroke associated with NSAIDs, except for aspirin. Remember: just because NSAIDs are available over-the-counter, they are still drugs with side effects and they can harm you when they are not used appropriately.
Every day in the news we hear about the abuse of pain medicines and other controlled substances. The Centers for Disease Control and Prevention, or CDC, reports escalating deaths of almost 72,000 in 2019 and 2020, exceeding deaths due to motor vehicle accidents. The majority of these deaths are due to illicit drugs. In reality, with decreasing prescriptions of opioids, prescription opioid deaths are decreasing. This may also facilitate illicit drug use. The authorities, physicians, and public-at-large are concerned. Consequently, we have new regulations on a daily basis coming from federal and state legisla–tures and agencies. Opioid use in America has been described as an epidemic. As a country we consume 99% of the world supply of hydrocodone and 50% of the oxycodone. So many drugs are prescribed in the United States that each and every person can have a 1 month supply of opioids.
Pain medications are known as opioids. The most common ones are hydrocodone and oxycodone and go by brand names such as Norco, Percocet, OxyContin, and many others.
The second group of drugs are called benzodiazepines, or anxiety medications. These include Valium, Xanax, Ativan, and Klonopin. These drugs in combination with opioids are considered as more addictive and dangerous.
The worst combinations are opioids, benzodiazepines, and some of the muscle relaxants.
Similar to wrists and knees, our spines also have joints called facets that cause pain in the neck, head, and back from arthritis or strain.
Facet joint pain is one of the most common pain symptoms with neck, mid back, and low back pain (Fig. 1). These major structures in the spine, on each side of a vertebral body, allow us to bend forward, backward, and side to side.
Facet joints can cause pain secondary to arthritis, degenera–tion, and also sprain and strain. Facet joint pain can be diagnosed with diagnostic facet joint nerve blocks, performed by injecting a local anesthetic over the nerve supply of the joint.
An epidural injection delivers medication into the epidural space around the spinal nerve roots to relieve pain caused by irritated spinal nerves. These injections generally include local anesthetics and steroids and occa–sionally other substances; to reduce the inflammation of the nerves.
With an interlaminar approach to epidural injection, the needle is placed in the center of the spine between 2 vertebral bodies and the epidural space is entered under fluoroscopic visualization. However, in the low back, there are 2 other types of epidural injections. A caudal epidural injection is performed by entering through the small opening above the tailbone called the sacral hiatus. This approach is best in patients after having low back surgery. Another mode of treatment is called a transforaminal epidural injection. With this approach, the needle is placed close to the origin of the nerve root.
All epidural injections may be associated with very small risk. Steroids also may have problems related to weight gain, loss of bone density, immunosuppression, flushing, and an increase in blood sugar.
Epidural injections may be helpful initially for 3 to 6 weeks, and after the third injection, approximately for 3 months or
longer each time if patients are selected and an appropriate response is obtained.
A spinal cord stimulator is an electrical nerve stimulation device implanted into your body to control chronic pain. It is indicated for the failure of surgery in the low back, for severe nerve-related pain or numbness, and for complex regional pain syndrome after all other treatments have failed.
Spinal cord stimulation consists of stimulating electrodes implanted in the epidural space, an electrical pulse generator implanted in the lower abdominal area or gluteal region, wires connecting the electrodes to the generator, and the generator’s remote control.
A spinal cord stimulator is an electrical nerve stimulation device implanted into the body in 2 stages to control chronic pain. It is indicated for the failure of surgery in the low back for severe nerve related pain or numbness and for complex regional pain syndrome after all other treatments have failed. Spinal cord stimulation consists of stimulating electrodes implanted in the epidural space and an electrical pulse generator implanted in the lower abdominal area or gluteal region. Spinal cord stimulation may be effective in approximately 50% to 60% of patients after all other modalities have failed.
Regenerative medicine broadly describes an innovative medical therapy that will enable the body to repair, replace, restore, and regenerate damaged or diseased cells, tissues, and organs. Regenerative medicine represents a new paradigm in human health because the vast majority of treatments for chronic and life-threatening diseases focus on treating the symptoms, not curing the disease. Regenerative medicine is mainly based on cellular therapies which amplify our natural healing process in the place it is needed most, or take over function of a permanently damaged organ.
Regenerative medicine is a new field, specifically in managing chronic pain. Regenerative medicine with stem cell therapy is much advanced in other areas. The devel–opments in chronic pain management include the use of platelet rich plasma, or PRP, and adult stem cells to help build healthy discs, tendons, cartilage, ligaments, and bone. PRP is obtained by drawing your own blood, and then spinning it in a centrifuge to separate a concentrated layer of platelets from the red blood cells. This layer of PRP from the patient’s own blood is then injected into or around the injured site. PRP contains growth factors and cells that enhance and strengthen the body’s ability to generate healthy tissue. The injection is carried out under image guidance to ensure accuracy.
The other part of regenerative medicine in chronic pain is stem cells obtained from the patient’s bone marrow or fat. Similar to PRP, stem cells are also injected into or around the injured site under image guidance.
At PMCA, we provide regenerative medicine utilizing current principles under image guidance.